effi-science/e-sciences
La chondroïtine
1. La chondroïtine: qu’est ce que c’est ?
La chondroïtine est une molécule employée en traitement dans l’arthrose. Comme la glucosamine, elle est de la classe des “traitements symptomatiques à action lente”, des molécules qui vont avoir un effet en profondeur sur l’arthrose.
A. La chondroïtine naturellement présente dans l’organisme
Au sein de l’articulation, les chondrocytes sont les cellules responsables de la formation du cartilage et la destruction du cartilage usé, ainsi que de la synthèse de la glucosamine et la chondroïtine.
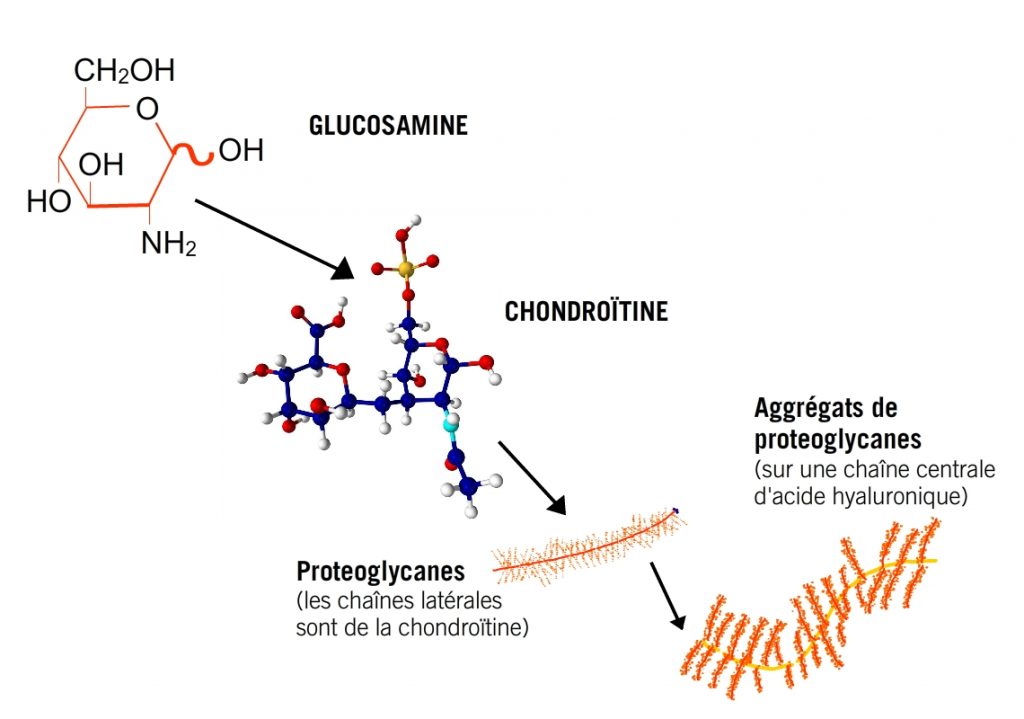
Ce sont les chondrocytes qui vont former la chondroïtine, elle est assemblée comme une chaîne à partir de plus petits éléments. Ensuite, ces chaînes de chondroïtine vont être assemblées en plus grands éléments, les protéoglycanes, et ensuite ceux-ci vont eux-mêmes aussi être rassemblés Ces protéoglycanes vont attirer et fixer les molécules d’eau et faire en sorte que l’articulation soit bien lubrifiée et puisse absorber les chocs.
B. Les suppléments de chondroïtine
La chondroïtine est employée comme complément alimentaire pour soulager les articulations. Comme c’est une molécule assez grande, le corps va devoir la diviser avant de pouvoir l’absorber, c’est pourquoi son absorption n’est en général pas très haute (10-20%) [1]. Ensuite elle est transportée dans le sang et se concentre dans le liquide synovial et le cartilage. La chondroïtine employée par E-sciences provient de la trachée de bovins. Longtemps la chondroïtine a été extraite de requins et de raies, mais les méthodes pour récolter celle-ci sont peu écologiques: les ailerons sont découpés et les requins rejetés vivants à la mer.
La provenance des bovins est très bien contrôlé, et le cartilage est récupéré lors du processus d’abattage pour la viande.
Il est important de prendre la chondroïtine en dosage suffisant: 1200 mg / jour. Il est aussi important de prendre la bonne quantité tous les jours, afin qu’il y ait une dose constante dans l’organisme. Aussi, la chondroïtine est un médicament d’action lente, donc les effets ne peuvent être évalués que après 3 à 6 mois.
2. Arthrose et chondroïtine : comment ça marche ?
La chondroïtine va agir sur les deux aspects de l’arthrose: l’usure du cartilage et la cascade inflammatoire [2].
Les molécules de chondroïtines ne rentrent pas dans les cellules de l’articulation (chondrocytes, ostéoblastes etc) mais leurs effets se font via des récepteurs sur les membranes de ces cellules [1]. Ces effets peuvent être divisés en deux grandes catégories:
A. Effets sur le cartilage
B. Effets sur la cascade inflammatoire
A. Effets sur le cartilage
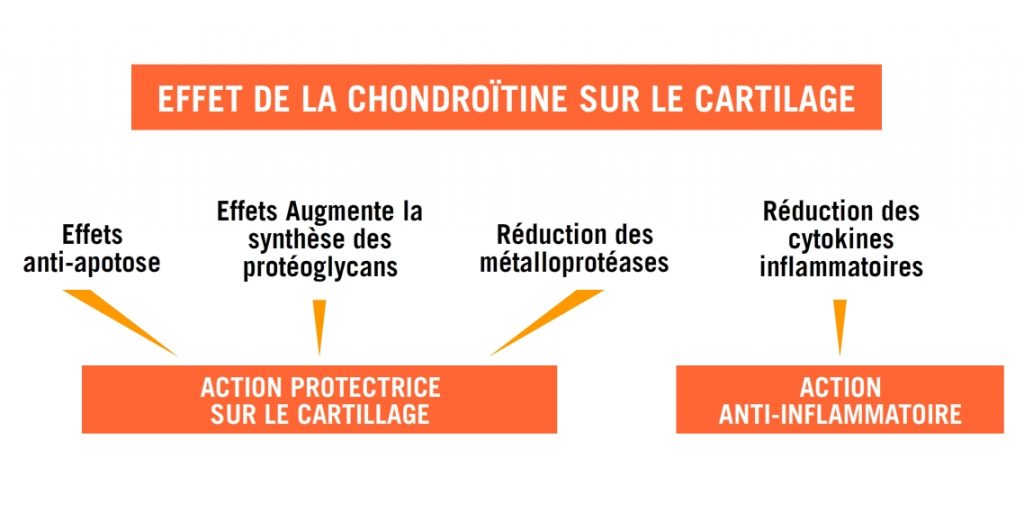
La chondroïtine a trois effets distinct qui maintiennent la bonne santé du cartilage :
– effet anti-apoptose
– permettre aux chondrocyte de créer plus de protéoglycanes
– empêcher les métalloprotéases de les dégrader.
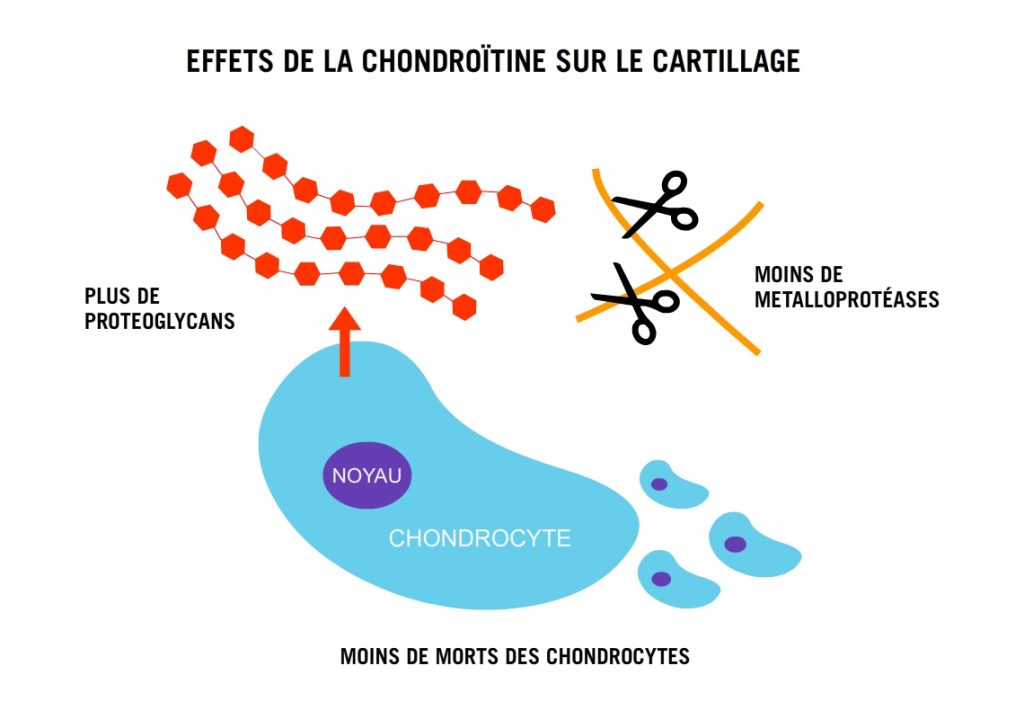
1. Effet anti-apoptose
Le mauvais renouvellement du cartilage est en partie la conséquence d’une mort trop importante des cellules qui fabriquent le cartilage, les chondrocytes.
Lorsqu’une cellule est usée, elle est éliminée de façon programmée: ce procédé se nomme apoptose (si la mort de la cellule n’a pas lieu de façon programmée on parlera plutôt de lyse ou de nécrose). Dans l’arthrose le processus d’apoptose est déréglé, les enzymes responsable de la mort des cellules sont suractivés. La chondroïtine permet de réguler ces enzymes et empêche donc la mort des cellules.
2. Augmente la synthèse des protéoglycans
Un supplément de chondroïtine “livre” des briques avec lequel l’organisme peut constituer de nouveaux protéoglycans, composants essentiels du cartilage.
3. Réduction des métalloprotéases
Les métalloprotéases sont les enzymes qui vont détruire des éléments du cartilage et de la matrice articulaire. En effet, le corps doit pouvoir se débarrasser des composants usés. Par contre, dans le cadre de l’arthrose ces enzymes sont présent en trop grandes quantités. Les cytokines inflammatoires stimulent les cellules du cartilage à produire plus de protéases, donc la destruction des composants est augmenté. Les métalloprotéases sont contenues par des inhibiteurs, les TIMPs. La chondroïtine va signaler à la cellule d’augmenter le nombre de TIMPS, qui vont donc empêcher les métalloprotéases de nuire.
B. Effets sur la cascade inflammatoire
La cascade inflammatoire est un phénomène complexe ou des tas de molécules vont en induire d’autres, mettre en marche des systèmes complexes, créer des dérèglements, etc.
Un des grands coupables dans les problèmes d’arthrose est la cytokine pro-inflammatoire interleukine-1-bèta (ou IL-1β).
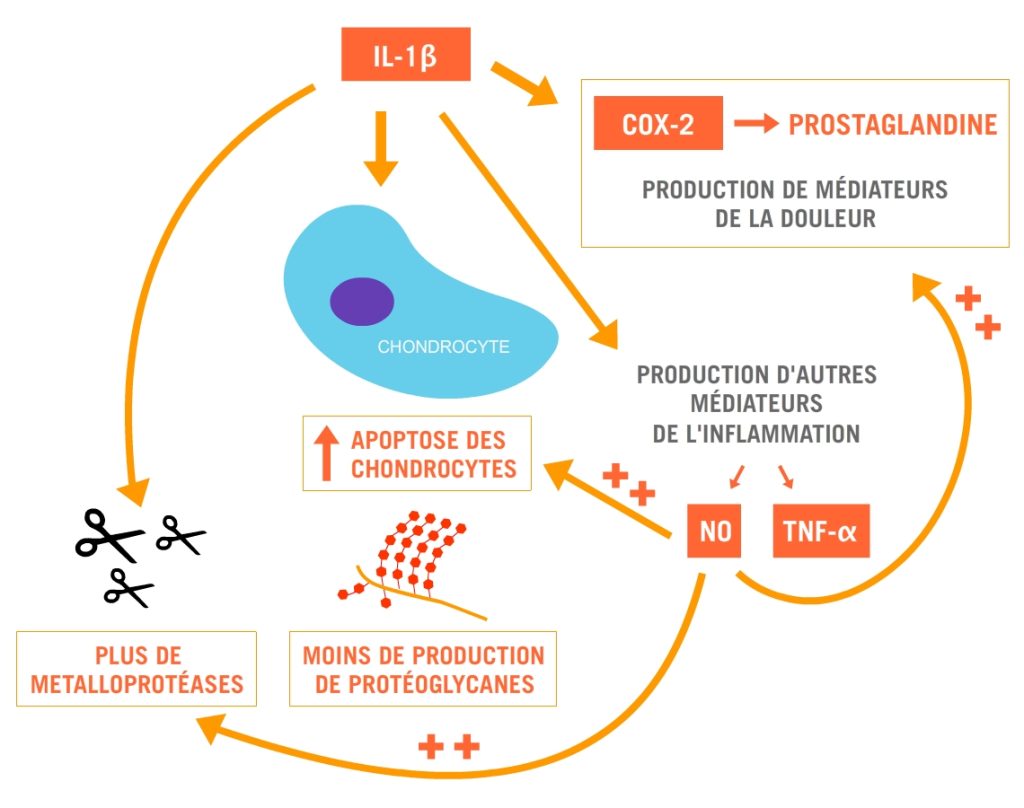
L’IL-1β est donc responsable de plusieurs effets, à différents niveaux :
– augmentation de la mort des chondrocytes
– activation des enzymes COX-2 et donc production de prostaglandines responsables de la sensation de douleur (plus d’info ici )
– augmentation de la synthèse de métalloprotéases
– diminution de la synthèse de protéoglycanes
En plus de cela, l’IL-1β déclenche d’autres cytokines comme le NO (oxide nitrique) et le TNF-α (tumor necrosis factor alpha), qui vont venir renforcer ses effets.
Nous avons déjà vu que la chondroïtine va agir niveau du cartilage, mais en plus de ça elle va également empêcher la production de NO et inhiber l’activation des COX-2
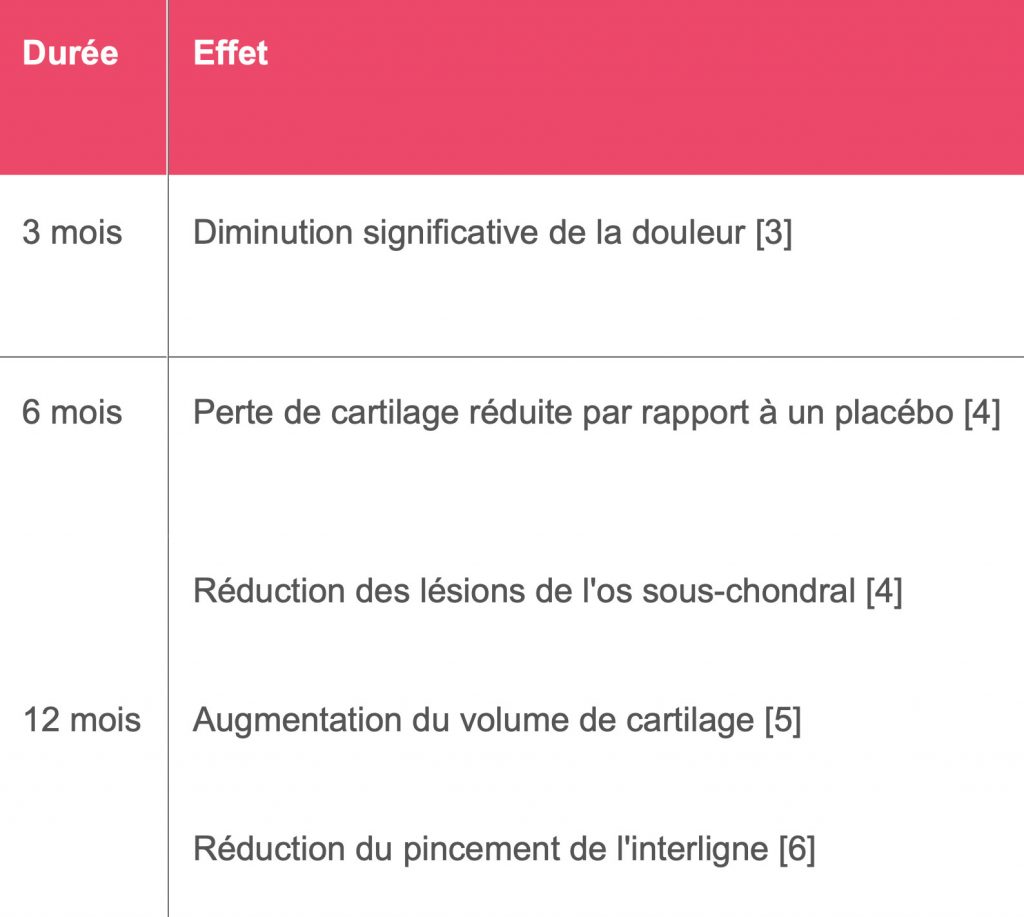
3. Effets de la chondroïtine

Cartilamine Chondro
Cartilamine Chondro est recommandé en cas de gêne articulaire plus intense que dans le cas décrit pour Cartilamine 1500. Il est adapté à une forte dégradation du cartilage.
A partir de 21,90€
[1] Du Souich, Patrick. 2014. “Absorption, Distribution and Mechanism of Action of SYSADOAS.” Pharmacology & Therapeutics 142 (3) (June): 362–74.
[2] Henrotin, Yves, Mariane Mathy, Christelle Sanchez, and Cecile Lambert. 2010. “Chondroitin Sulfate in the Treatment of Osteoarthritis: From in Vitro Studies to Clinical Recommendations.” Therapeutic Advances in Musculoskeletal Disease 2 (6) (December): 335–48.
[3] ZEGELS B, et al. 2013. “Equivalence of a Single Dose (1200 Mg) Compared to a Three-Time a Day Dose (400 Mg) of Chondroitin 4&6 Sulfate in Patients with Knee Osteoarthritis. Results of a Randomized Double Blind Placebo Controlled Study.” Osteoarthritis and Cartilage / OARS, Osteoarthritis Research Society 21 (1) (January): 22–7.
[4] WILDI L.M., et al. 2011. “Chondroitin Sulphate Reduces Both Cartilage Volume Loss and Bone Marrow Lesions in Knee Osteoarthritis Patients Starting as Early as 6 Months after Initiation of Therapy: A Randomised, Double-Blind, Placebo-Controlled Pilot Study Using MRI.” Annals of the Rheumatic Diseases 70 (6) (June): 982–9.
[5] RAILHAC J-J, et al. 2012. “Effect of 12 Months Treatment with Chondroitin Sulfate on Cartilage Volume in Knee Osteoarthritis Patients: A Randomized, Double-Blind, Placebo-Controlled Pilot Study Using MRI.” Clinical Rheumatology 31 (9) (September): 1347–57.
[6] UEBELHART D, et al. 2004. “Intermittent Treatment of Knee Osteoarthritis with Oral Chondroitin Sulfate: A One-Year, Randomized, Double-Blind, Multicenter Study versus Placebo.” Osteoarthritis and Cartilage / OARS, Osteoarthritis Research Society 12 (4) (April): 269–76.